Weight training without shoulder injuries
Authors:
Durall CJ, Manske RC, Davies GJ.
Translation
Sergei Strukov.
One of the main responsibilities of a personal trainer or strength and conditioning specialist is to teach clients proper exercise technique. However, what is more important to the strength and conditioning professional is the ability to develop training programs that are safe and appropriate for the client. Because there are many exercises for each muscle or muscle group, it is wise to avoid exercises that are likely to cause injury.
Shoulder injuries are relatively common among weight trainees and can be career-destroying at the competitive level (14, 26). Fortunately, most shoulder injuries from resistance training are mild musculotendinous or ligamentous-capsular tears. However, the use of inappropriate exercises or techniques aggravates the situation or contributes to the development of glenohumeral joint instability (19, 21) or impingement (8, 9, 12, 16).
In this article, we will identify common exercises that contribute to or aggravate glenohumeral joint injuries. Alternative options and rationale for replacement exercises are described. A comprehensive review of undesirable exercises for known shoulder pathologies is not the purpose of the article: only pathologies associated with strength training are discussed. Avoiding hazardous exercise will help prevent injury in healthy clients and further tissue damage in people recovering from injury.
Features[edit | edit code]
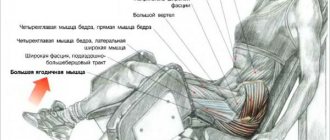
Infraspinatus muscle
(
m. infraspinatus
) participates in the formation of the rotator cuff and, weaving into the capsule of the shoulder joint, strengthens it. The infraspinatus muscle is considered a strong external rotator of the shoulder, especially in the final phase, when with external rotation of the greater tuberosity and continued abduction of the arm it is necessary to avoid its impact with the roof of the shoulder joint. The cranial part of this muscle abducts the arm, and the caudal part adducts.
| Functions | Synergists | Antagonists |
| Shoulder external rotation | *M. teres minor *M. deltoideus (spinous part) | *M. pectoralis major *M. deltoideus (clavicular part) *M. latissimus dorsi *M. teres major *M. biceps brachii |
| Shoulder adduction | *M. pectoralis major *M. latissimus dorsi *M. teres major *M. teres minor *M. coracobrachialis *M. biceps brachii (short head) *M. deltoideus (spinous and clavicular parts with the arm already adducted) *M. triceps brachii (long head with arm already abducted) | *M. deltoideus (acromial part) *M. deltoideus (spinous and clavicular parts with the arm abducted) *M. infraspinatus (cranial part) *M. biceps brachii (long head) |
| Shoulder abduction | *M. deltoideus (acromial part) *M. deltoideus (spinous and clavicular parts with the arm abducted) *M. biceps brachii (long head) | *M. pectoralis major *M. latissimus dorsi *M. teres major *M. teres minor *M. coracobrachialis *M. biceps brachii (short head) *M. deltoideus (clavicular and spinous parts with the arm already adducted) *M. infraspinatus (caudal part) *M. triceps brachii (long head with arm already abducted) |
| Shoulder retroversion with the arm abducted | *M. deltoideus (spinous part) *M. teres minor | *M. pectoralis major *M. deltoideus (clavicular part) *M. coracobrachialis *M. biceps brachii (short head) |
Shoulder external rotation. Functional muscle tests[edit | edit code]
Issues and comments
- With this test, it is almost impossible to distinguish between the functions of the teres minor, infraspinatus muscles and the acromial part of the deltoid muscle.
- If the arm is extended, supination at the elbow may appear as external rotation.
- Due to the more superficial location of the latissimus dorsi muscle, it is not always possible to palpate the infraspinatus muscle.
Symptoms
• Sudden sharp pain in the upper arm. • Sometimes a clearly audible cracking or crunching sound. • Contractions of the biceps muscle during intense movements of the arm. • Bruises extending from the middle of the shoulder down to the elbow. • Pain or tenderness in the shoulder and elbow area. • Weakness in the shoulder or elbow. • Difficulty turning the hand palm down or palm down. • Because the torn tendon can no longer hold the muscle under tension, a bulge above the elbow may appear in the arm, with a simultaneous concavity near the shoulder (Popeye's sign).
Participation in sports[edit | edit code]
As a strong external rotator of the shoulder, this muscle plays an important role in fencing. When playing sports, its cranial part performs both static (archery) and dynamic (fencing, weightlifting) work. The infraspinatus muscle is active in all sports that require retroversion of the arm from an anterior or lateral position (archery, tennis, discus throwing).
| Kind of sport | Movement/hold | Function | Load | Types of abbreviations |
| Fencing | Rotational movements with weapons | Shoulder external rotation | Fast | Dynamic concentric |
| Lunge | Shoulder abduction | Fast, explosive | Dynamic concentric | |
| Archery | Stabilizing the bow hand | Shoulder abduction | Strength endurance | Static |
| Weightlifting | Thrust phase | Shoulder abduction | Fast, explosive, maximum | Dynamic concentric |
| Archery | Pulling the bowstring | Retroversion of the arm from a front or side position | Strength endurance | Dynamic concentric |
| Tennis | Backhand | Retroversion of the arm from a front or side position | Fast, explosive | Dynamic concentric |
| Discus throw | Hand return | Retroversion of the arm from the side position | Strength endurance | Dynamic concentric |
Science that studies the body
In this regard, the concepts of “fascia” and “myofascial chains” also appeared. The science that directly deals with the health of the human body is called kinesiology. From “kinesio” - movement, “logos” - to study. That is, she studies the patterns of body movement.
This may be applicable in sports, in the treatment of pathologies, massage therapists and chiropractors may be interested in this. There are not many kinesiologists, but more and more modern doctors - osteopaths, neurologists - are interested in this area.
Read also[edit | edit code]
- Muscles - anatomy and functions
- Muscles of the shoulder girdle
- Arm muscles
- Shoulders - exercises and training features
- Anatomy of the shoulder joint
- Trapezius muscle
- Levator scapulae muscle
- Rhomboid muscles
- Serratus anterior muscle
- Deltoid
- Supraspinatus muscle
- Subscapularis muscle
- Latissimus dorsi muscle
- Teres major muscle
- Teres minor muscle
- Pectoralis major muscle
- Pectoralis minor muscle
- Subclavius muscle
- Coracobrachialis muscle
What do we have to do?
Before you begin, assess your current range of motion. This will help you track your progress. A doctor or trainer can help with this.
First you need to warm up your arms and shoulders. This can be achieved by regular stretching. After this, you can move on to strengthening exercises.
Stretch 1
Extend your right arm to the left across your chest. Grasp the shoulder of your right hand with your left palm. Hold the position for 30 seconds, then do the same with the other hand.
Stretch 2
Raise your right arm above your head and bend it behind your neck. Grasp the elbow of your right hand with your left palm. Hold the position for 30 seconds, then do the same with the other hand.
Stretch 3
Stand straight with your legs slightly apart to perform pendulum movements. Lean forward, arms hanging parallel to your legs. Relax your arm and shoulder muscles and swing your arms slowly back and forth. Perform for 30 seconds.
Stretch 4
Start in a standing position with your legs slightly apart. Take one end of the folded towel in your right hand. Raise your right arm above your head and lower it behind your back. Place your left hand behind your back, bend it and grab the free edge of the towel. Hold the position for 30 seconds, then do the same with the other hand. Do it 3 times. Over time, try to reduce the distance between the brushes. In the end, you will be able to do without a towel and bring the brushes together. The closer you are to this result, the greater your shoulder flexibility.
Stretch 5
Lean your right side against the wall. Place your right hand along the wall behind your back at 90°. Turn your palm inward and hold for 30 seconds. Turn your palm outward and hold for 30 seconds. Repeat the same with the other hand.
Exercise 1
Lie on your right side on a table or bed. The right arm should be extended above the head, the head resting on the arm. Place a folded towel under your right armpit. Place your left arm along your body and bend it at the elbow 90°. In this case, the left forearm should be perpendicular to the body, with the palm facing the floor. Keeping your elbow bent, raise your arm up. Hold for 2-3 seconds, then return your hand to the starting position. Repeat and do the same with the other hand.
Exercise 2
Lie on your right side on a table or bed. The right arm should be extended above the head, the head resting on the arm. Place a folded towel under your right armpit. Place your left arm along your body and bend it at the elbow 90°. In this case, the left forearm should be perpendicular to the body, with the palm facing the floor. Keeping your elbow bent, lower your arm down. Hold for 2-3 seconds, then return your hand to the starting position. Repeat and do the same with the other hand.
Exercise 3
Lie on your right side on a table or bed. The right arm should be extended above the head, the head resting on the arm. Place a folded towel under your right armpit. Place your left arm along your body and bend your elbow 90°. In this case, the left forearm should be perpendicular to the body, with the palm facing the floor. Without lifting your elbow from your body, raise your left forearm to its maximum. (The movement of the forearm should be away from the body.) Hold for 2-3 seconds, then return your hand to the starting position. Repeat and do the same with the other hand.
Exercise 4
Lie on your right side on a table or bed. The right arm should be extended above the head, the head resting on the arm. Place a folded towel under your right armpit. Place your left arm along your body and bend your elbow 90°. In this case, the left forearm should be perpendicular to the body, the palm facing the floor. Keeping your left shoulder in place, raise your entire left arm to at least 45 degrees. The elbow remains bent throughout the entire range of motion. Hold for 2-3 seconds, then return your hand to the starting position. Repeat and do the same with the other hand.
A set of exercises after shoulder arthroplasty
Postoperative rehabilitation plays a vital role in restoring daily activities after shoulder surgery. Follow your surgeon's instructions and work hard to achieve the best result.
Early rehabilitation.
Stretching and normal daily activities usually begin on the day of surgery. At your request, pain relief therapy can be prescribed. First of all, under the supervision of a rehabilitation physician, gentle rocking movements in the shoulder begin, giving the shoulder different positions to relax the muscles. These passive exercises help prevent stiffness while movement in the shoulder gradually returns. You also need to tense the muscles in your hand and forearm by flexing your wrist and elbow.
A rehabilitation doctor will show you the safest ways to get up and down in bed, sit on a chair or toilet. The rehabilitation therapist will track your daily progress and keep your surgeon updated.
Causes of biceps tendon rupture
It is worth noting that regular physical exercise, and not occasionally, can strengthen tendon tissue. There are no other effective ways to strengthen tendons (with the possible exception of prolotherapy, which is in clinical research). It is worth noting that even if prolotherapy turns out to be effective, its implementation in relation to the proximal tendons of the biceps brachii muscle will be very difficult. Various biological additives also do not have real effectiveness, and recommendations for abundant consumption of jellied meat, meat broths, and chicken cartilage are nothing more than widespread myths.
Additional risk factors for biceps tendon ruptures include:
- Smoking: Nicotine can interfere with the nutrition of tendon tissue.
- Administration of corticosteroids. Taking and local injections of corticosteroids (drugs such as diprospan, hydrocortisone) can cause necrosis and tendon rupture.
- In addition, there are suggestions that certain systemic diseases and the use of fluoroquinolone antibiotics may contribute to tendon rupture.
Subcutaneous biceps brachii tears occur primarily as a result of indirect trauma. A sharp sudden contraction of a muscle in a state of tension leads to rupture of the long head tendon during impact, wrestling, lifting of weights and the distal tendon, mainly during sudden lifting of weights. A complete rupture leads to the formation of diastasis between the ends of the tendon due to both muscle traction and degenerative changes in the ends of the damaged tendon. Depending on the size of the diastasis, tendon ruptures are divided into:
- small (up to 1 cm),
- medium (from 1 to 3 cm),
- large (from 3 to 5 cm),
- and extensive (over 5 cm).