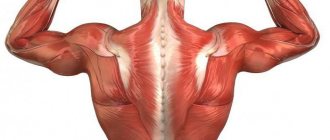
Good afternoon Today we will look at the anatomy of the chest muscles. This is one of the simplest and most understandable topics in myology - the branch of anatomy that examines the structure and location of muscles.
The first thing we need to remember is classification. Here it is very simple, and if you have ever gone to the gym at least once in your life, you will immediately understand the principle of this classification. If you’ve never gone, you’ll also understand that this is not a problem (although, of course, sports are cool).
The chest muscles are divided into superficial muscles associated with the upper limb, and deep muscles - that is, the own chest muscles. What does it mean?
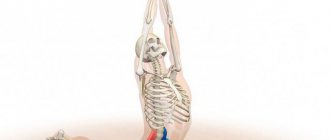
One of the basic exercises with barbells is the bench press. The athlete lies down on the bench, removes the barbell from its fastenings, and then pushes it upward by straightening the arms bent at the shoulder and elbow joints.
As you can see, the upper limbs bend and extend. And the load falls on the chest muscles (we’ll figure out which ones later). This is an excellent illustration of the classification - we see muscles that seem to be located in the chest area, but they do not move the chest, but the upper limb.
As you remember, the skeleton of the upper limb consists of the bones of the upper limb girdle (these are the scapula and the collarbone) and the bones of the free upper limb (this is actually the arm).
The superficial muscles of the chest are anatomically connected to the upper limb - either to the belt, or to the arm. The deep muscles of the chest, they are also your own, are in no way connected with the upper limb; they are located directly in the chest area.
Function
Pulls the shoulder blade forward, down and inward, raising the ribs. Synergists are the pectoralis major muscle (lowering the shoulder, retracting the scapula and rotating its outer angle down) and the latissimus dorsi muscle (lowering the shoulder). The antagonists are the rhomboid muscle and the lower trapezius.
It is also an additional inspiratory muscle together with the levator scapulae, trapezius, sternocleidomastoid and scalene muscles (joint elevation of the ribs with a fixed scapula).
Respiratory muscles
External and internal intercostal muscles
There are two types of intercostal muscles: internal and external. The external ones are located under the superficial muscles, filling all the intercostal spaces of the anterior sections, in a more understandable language, these muscles are located directly on the ribs themselves in front, behind and between them. They are not located strictly vertically, but at an angle towards the chest. The external muscles begin from the lower edges of the upper rib and end at the upper edges of the underlying ribs. Main functions : raise the ribs, providing inspiration.
The internal intercostal muscles are also located between the ribs, but they are located inside the chest. In the area where cartilage is located, they are absent; there they are replaced by intercostal membranes. Main functions: lower the ribs and participate in the act of calm breathing. When breathing intensely, for example while running, other chest muscles are activated to exhale: the major and minor muscles, the trapezius, the neck and the abs.
Subcostal muscles
They are the deepest muscles of the chest, located below the internal intercostal muscles, attached to the ribs from below, on the inside. They differ from the intercostal muscles in that their bundles are thrown over one rib, reminiscent of basket weaving. Main functions: participate in the breathing process (exhalation). May raise the ribs during intense breathing.
Diaphragm
One of the unpaired muscles (does not have a pair). Separates the chest and abdominal cavities from each other, resembles a jellyfish in shape, begins along the entire circumference of the lower ribs, tapering towards the center and passes into the tendons. Main functions: during contraction, the diaphragm increases the volume of the chest and inhalation occurs. When relaxed, it takes on a convex shape (resembling a sphere). As a result, the chest shrinks and exhalation occurs. Also, involuntary jerky contractions lead to hiccups.
Pathology
Tunnel syndrome of the pectoralis minor muscle (Wright-Mendlovich syndrome) can occur when it is hypertonic and shortened. The pathologically altered muscle compresses the neurovascular bundle passing in close proximity to it. The causes of this syndrome are most often increased muscle loads and frequent repetitive movements with abduction of the arm to the side and rotation outward, due to which the muscle fibers are torn and damaged, followed by hypertonicity, shortening and hypertrophy.
Symptoms include chest pain in the projection of the muscles, radiating to the shoulder and hand to the fingers, as well as paresthesia along the limb. The syndrome is diagnosed based on specific tests by a neurologist or a specialist in musculoskeletal medicine (manual therapy). The treatment uses methods of novocainization, PIR, myofascial release and positional treatment.
Key exercises for chest training
The following exercises are the best for building strong and massive pectoral muscles.
Exercise 1 Incline Bench Press
Keep your leg and abdominal muscles tense throughout the exercise. When lifting dumbbells, do not place your elbows out to the sides as this will put more stress on your shoulders.
Although this exercise works all 3 parts of the pectoralis major muscles, it places a special load on the clavicular part. If for some reason you cannot pump up your upper chest, then add the incline bench press and dumbbell lateral raises to your training program.
If you experience shoulder discomfort while performing this exercise, use a neutral grip (palms facing each other). This will reduce the stress on your shoulders and make the exercise more comfortable.
Exercise 2 Lying dumbbell flyes
This exercise is the best for building chest muscles and performing horizontal adduction. Keep your abdominal, back and leg muscles tense. Maintain a slight bend in your elbows. By spreading your arms out to the sides, stretch your chest muscles.
When you bring your hands together, they will contract again. This exercise works all 3 parts of the pectoralis major muscles evenly.
Literature
- R. D. Sinelnikov, Ya. R. Sinelnikov
. Atlas of human anatomy. - 2nd. - M.:: Medicine, 1996. - M. G. Prives, N. K. Lysenkov, V. I. Bushkovich
. Human anatomy. — 11th edition. - St. Petersburg:: Hippocrates, 1998. - Hanz Fenish
. Pocket atlas of human anatomy. Minsk: Higher School, 1996. - M. R. Sapin, Z. G. Bryksina
. Human anatomy. M: Academy, 2008 - Lobzin V.S., Rakhimdzhanov A.R. and Zhulev E.M.
Tunnel compression-ischemic neuropathies, Tashkent, 1984
| Deep (muscles of the spine) | Erector spinae (Iliocostalis Longissimus Spinalis) Transverse spinalis (Semispinalis Multifidus Rotator muscles) Interspinous muscles Intertransverse muscles |
| Deep | External intercostal muscles Internal intercostal muscles Innermost intercostal muscles Subcostal muscles Transversus thoracis Levator ribs |
| Diaphragm | Lumbar part Rib part Sternum part |
| Muscles of the anterior abdominal wall | Rectus abdominis · Pyramidalis |
| Muscles of the posterior abdominal wall | Quadratus lumborum muscle |
| This is a draft article on anatomy. You can help the project by adding to it. |
Superficial chest muscles
It is very important to understand that one way or another the function of these muscles will be associated not with the chest, but with the upper limb. This is a distinctive feature of the entire superficial muscle group.
1. Pectoralis major muscle (musculus pectoralis major)
According to tradition, we start with the most noticeable muscle of the entire group, and in our case this is the pectoralis major muscle.
The outline of the pectoralis major muscle is very visible in people who love the aforementioned bench press. It is this exercise that makes the muscle powerful and noticeable, like Bane's. My regular readers probably know that I am partial to comics.
If you look at this frame without highlighting, you can clearly see the outline of the pectoralis major muscles:
Origin: the pectoralis major muscle begins from the clavicle, from the anterior surface of the sternum and cartilages of the 2-7 ribs, as well as from the anterior wall of the rectus abdominis sheath.
Insertion: greater tubercle of the humerus. As you can see, here there is the most important feature of all superficial muscles - attachment to the upper limb, in this case, to the arm. This is why push-ups, dips, and barbell presses put so much stress on the pectoralis major muscle.
Function: brings the hand to a sagittal position (as in the picture we have already looked at).
2. Pectoralis minor muscle (musculus pectoralis minor)
In the process of learning and memorizing the anatomy of the chest muscles, you must first learn the most important and noticeable one - the pectoralis major muscle.
Immediately below it you can find the pectoralis minor muscle. This muscle may only be visible after you move the pectoralis major muscle away during dissection, since the pectoralis minor muscle is directly underneath it. You won't be able to see it on a living person.
In this illustration, the pectoralis major muscle has been removed - and therefore the pectoralis minor muscle is very visible to us:
Origin: 3, 4, 5 ribs (the point where the bony part of the rib becomes cartilaginous).
Insertion: coracoid process of the scapula. Again we see how our pattern works - the muscle is attached to the bone of the upper limb girdle, which means it belongs to the superficial group of chest muscles.
Function: pulls the shoulder blade forward and lowers it down.
Subclavian muscle (musculus subclavius)
Once you have learned the two superficial pectoralis major and minor muscles, you can immediately remember the subclavian muscle - it is very simple.
We can't see it until we remove the pectoralis major muscle. But as soon as this large and massive muscle is removed, we see this beauty:
To find the subclavius muscle we need, we only need to find the collarbone itself. A thin strip that is located under the collarbone and almost parallel to it is the subclavian muscle.
Beginning: the cartilaginous part of the first rib (it goes, as it were, from bottom to top, from the first rib to the collarbone).
Insertion: acromial part of the clavicle.
Function: pulls the clavicle medially and downwards.
Serratus anterior (musculus serratus anterior)
When you look at different pictures and tablets of the chest muscles, you can see quite a lot of muscles that span or run along the ribs. Among all this incomprehensible mess of bones and meat, you need to be able to immediately identify the serratus anterior muscles. These muscles are the only muscles of the superficial group that run along several ribs.
What are their distinctive features? Let's label them.
- Surface position. These muscles are noticeable on a living person. The serratus anterior muscles are partially covered by the pectoralis major muscles, but beneath them the contours of the serratus anterior muscle are always clearly visible. You can see the outline of the serratus anterior muscle on Ezekiel Sims' body. This is one of the characters from the comic book "The Amazing Spider-Man".
- Bundles of the serratus anterior muscle cover the ribs rather than being located between them.
Beginning: outer surface of ribs 1-9 inclusive.
Insertion: medial edge and inferior angle of the scapula.
Function: pulls the scapula downward and laterally. The muscle also takes part in fixing the scapula to the surface of the chest.
A small life hack: when answering a test or exam about any muscle from this group, you can safely add the phrase “participates in the act of inhalation as an auxiliary muscle.” This is true - if you fix the attachment point of any superficial chest muscle, it will help you inhale.
Let's fill up our table:
Excerpt characterizing the pectoralis minor muscle
“De l'histoire ancienne, [Ancient history,"] said the other, guessing that it was about previous wars. - L'Empereur va lui faire voir a votre Souvara, comme aux autres... [The Emperor will show your Souvara, like others...] - Bonaparte... - Dolokhov began, but the Frenchman interrupted him. - No Bonaparte. There is an emperor! Sacre nom... [Damn it...] - he shouted angrily. - Damn your emperor! And Dolokhov swore in Russian, rudely, like a soldier, and, raising his gun, walked away. “Let’s go, Ivan Lukich,” he said to the company commander. “That’s how it is in French,” the soldiers in the chain spoke. - How about you, Sidorov! Sidorov winked and, turning to the French, began to babble incomprehensible words often, often: “Kari, mala, tafa, safi, muter, caska,” he babbled, trying to give expressive intonations to his voice. - Go Go go! ha ha, ha, ha! Wow! Wow! - there was a roar of such healthy and cheerful laughter among the soldiers, which involuntarily communicated through the chain to the French, that after this it seemed necessary to unload the guns, detonate the charges and everyone should quickly go home. But the guns remained loaded, the loopholes in the houses and fortifications looked forward just as menacingly, and just as before, the guns turned towards each other, removed from the limbers, remained. Having traveled around the entire line of troops from the right to the left flank, Prince Andrei climbed to the battery from which, according to the headquarters officer, the entire field was visible. Here he dismounted from his horse and stopped at the outermost of the four cannons that had been removed from the limbers. In front of the guns walked the sentry artilleryman, who was stretched out in front of the officer, but at a sign made to him, he resumed his uniform, boring walk. Behind the guns there were limbers, and further back there was a hitching post and artillery fires. To the left, not far from the outermost gun, there was a new wicker hut, from which animated officer voices could be heard. Indeed, from the battery there was a view of almost the entire location of the Russian troops and most of the enemy. Directly opposite the battery, on the horizon of the opposite hillock, the village of Shengraben was visible; to the left and to the right one could discern in three places, among the smoke of their fires, masses of French troops, of which, obviously, most of them were in the village itself and behind the mountain. To the left of the village, in the smoke, there seemed to be something similar to a battery, but it was impossible to get a good look at it with the naked eye. Our right flank was located on a rather steep hill, which dominated the French position. Our infantry was positioned along it, and the dragoons were visible at the very edge. In the center, where the Tushin battery was located, from which Prince Andrei viewed the position, there was the most gentle and straight descent and ascent to the stream that separated us from Shengraben. To the left, our troops adjoined the forest, where the fires of our infantry, chopping wood, were smoking. The French line was wider than ours, and it was clear that the French could easily get around us on both sides. Behind our position there was a steep and deep ravine, along which it was difficult for artillery and cavalry to retreat. Prince Andrei, leaning on the cannon and taking out his wallet, drew for himself a plan for the disposition of the troops. He wrote notes in pencil in two places, intending to communicate them to Bagration. He intended, firstly, to concentrate all the artillery in the center and, secondly, to transfer the cavalry back to the other side of the ravine. Prince Andrei, constantly being with the commander-in-chief, monitoring the movements of the masses and general orders and constantly engaged in historical descriptions of battles, and in this upcoming matter involuntarily thought about the future course of military operations only in general terms. He imagined only the following kind of major accidents: “If the enemy launches an attack on the right flank,” he said to himself, “the Kiev Grenadier and Podolsk Jaeger will have to hold their position until the reserves of the center approach them. In this case, the dragoons can hit the flank and overthrow them. In the event of an attack on the center, we place a central battery on this hill and, under its cover, pull together the left flank and retreat to the ravine in echelons,” he reasoned with himself...
Muscle strain
If a person is regularly exposed to physical activity on the pectoralis minor muscle, the process will lead to impaired functioning of the shoulder system. As a result, the risk of injury to this area as a result of lifting heavy objects or sudden movements increases significantly. The most common problem among patients is subacromial impingement syndrome. This is a condition in which there is not enough space for the muscle group between the humerus and the acromion. The disease leads to pinching of the tendon of the periosteum muscle, as well as the subacromial bursa. The syndrome is especially evident when lifting the limb above shoulder level and during rotational movement. Associated symptoms include the following:
- dull pain in the shoulder area;
- increased pain when raising your arms;
- crunching or clicking in the shoulder;
- limited mobility of the affected shoulder;
- weakness in the hand;
- problems with dreams due to pinched blood vessels and nerve fibers.
A negative process resulting from overstrain of the pectoralis minor muscle leads to pinching of nerve fibers, tendon tissue, arterial and venous vessels.
Patients are often diagnosed with hypertonicity of the pectoralis minor muscle. At the same time, the patient feels painful feelings. This is a condition in which when a muscle is loaded, it puts up a lot of resistance. This pathological condition leads to difficult movement and various symptoms. In order to restore physical activity, it is necessary to consult a doctor in a timely manner, undergo diagnostics and begin treatment. As a rule, patients are recommended therapeutic massages, physiotherapy, and gymnastic exercises. The sooner treatment is started, the easier it is to restore the body and prevent curvature of posture.